The problem
Genome-wide association studies link DNA to disease, and we have run them on millions of people.
As of 2021, about 86% of those people were of European ancestry. The clinical product, the
polygenic risk score, is several-fold less accurate outside that group. Middle Eastern and Gulf
populations are barely represented at all.
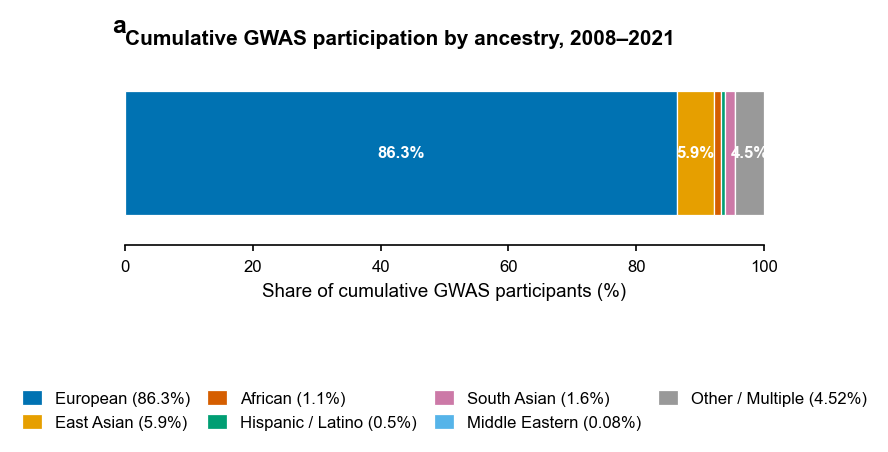
Figure 1. Cumulative GWAS participation by ancestry, 2008 to 2021. European ancestry makes
up roughly 86%, with most other groups close to the axis.
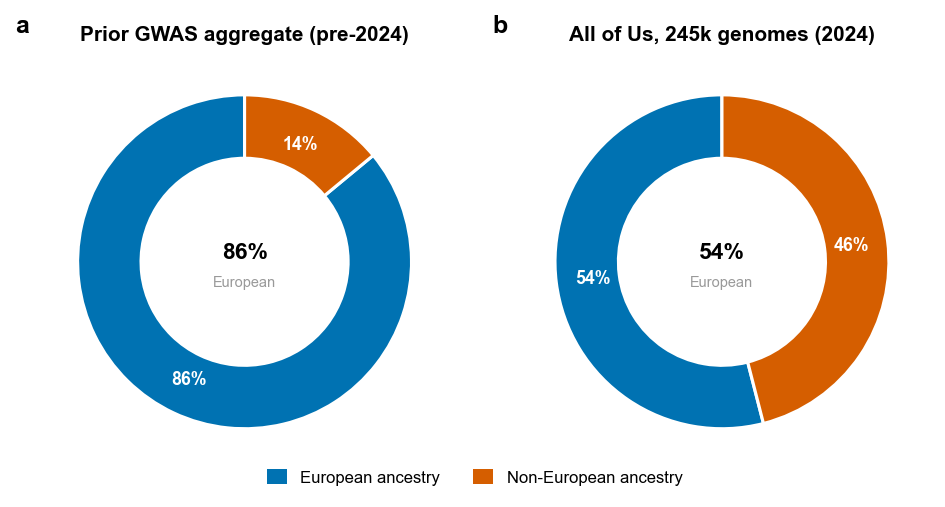
All of Us, and the figure that became the story
In 2024 the All of Us program published a landmark paper. It sequenced 245,000 genomes, about 46%
from non-European ancestry, which is a real step toward closing the gap. The cover charts show that
shift away from the old 86% European aggregate. Its headline figure was the problem. A UMAP
coloured by self-described race made a continuous genetic landscape look like a handful of discrete
races. The same paper also published an admixture plot showing the continuous reality, yet the
UMAP became the press image, and geneticists pushed back within weeks. Bias entered not only
through who was sampled, but through which figure reached the front page.
Why this matters for the Gulf
Even All of Us, with its 46% non-European cohort, includes almost no Middle Eastern ancestry. A
polygenic risk score trained on it will not transfer cleanly to an Emirati patient. That is why
the Emirati Genome Programme and the Qatar Genome Programme matter. Regional cohorts are a
precondition for safe genomic medicine here, not a redundant copy of the international ones.
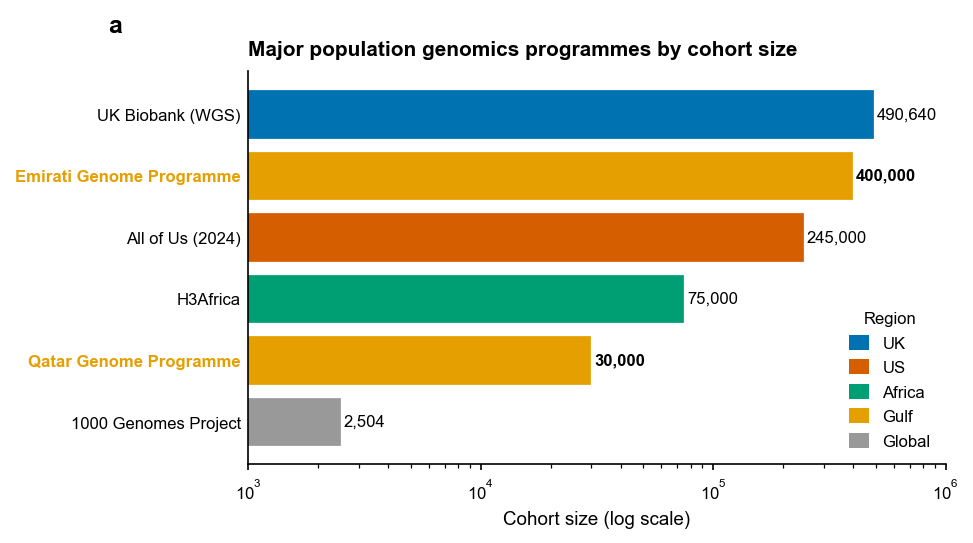
Figure 2. Major population genomics programmes by cohort size. The Gulf programmes are
building national reference genomes that international datasets do not cover.
Recommendations
The talk closes with five recommendations: treat ancestry as a continuum rather than fixed
categories, add a bias-and-equity review step for genomic publications, default Gulf clinical
tools to local reference data, train clinicians to read risk scores as ancestry-dependent
confidence intervals, and pre-register visualisation choices, not just analyses. The slides and the
full reference list are in the
repository.