The decision
After a heart attack and a stent, a patient needs an antiplatelet drug. The usual choice,
clopidogrel, does not activate well in people who are CYP2C19 poor or intermediate metabolisers,
who then stay at higher risk of another event. In a UAE pilot, about 47% of cardiovascular
patients carried such a phenotype. A single global prescribing rule cannot be assumed for a
population this mixed, which is the gap this plan addresses.
The pathway
The plan centres on that one prescribing decision and traces it across the people and systems
involved, from genetic testing through to follow-up.
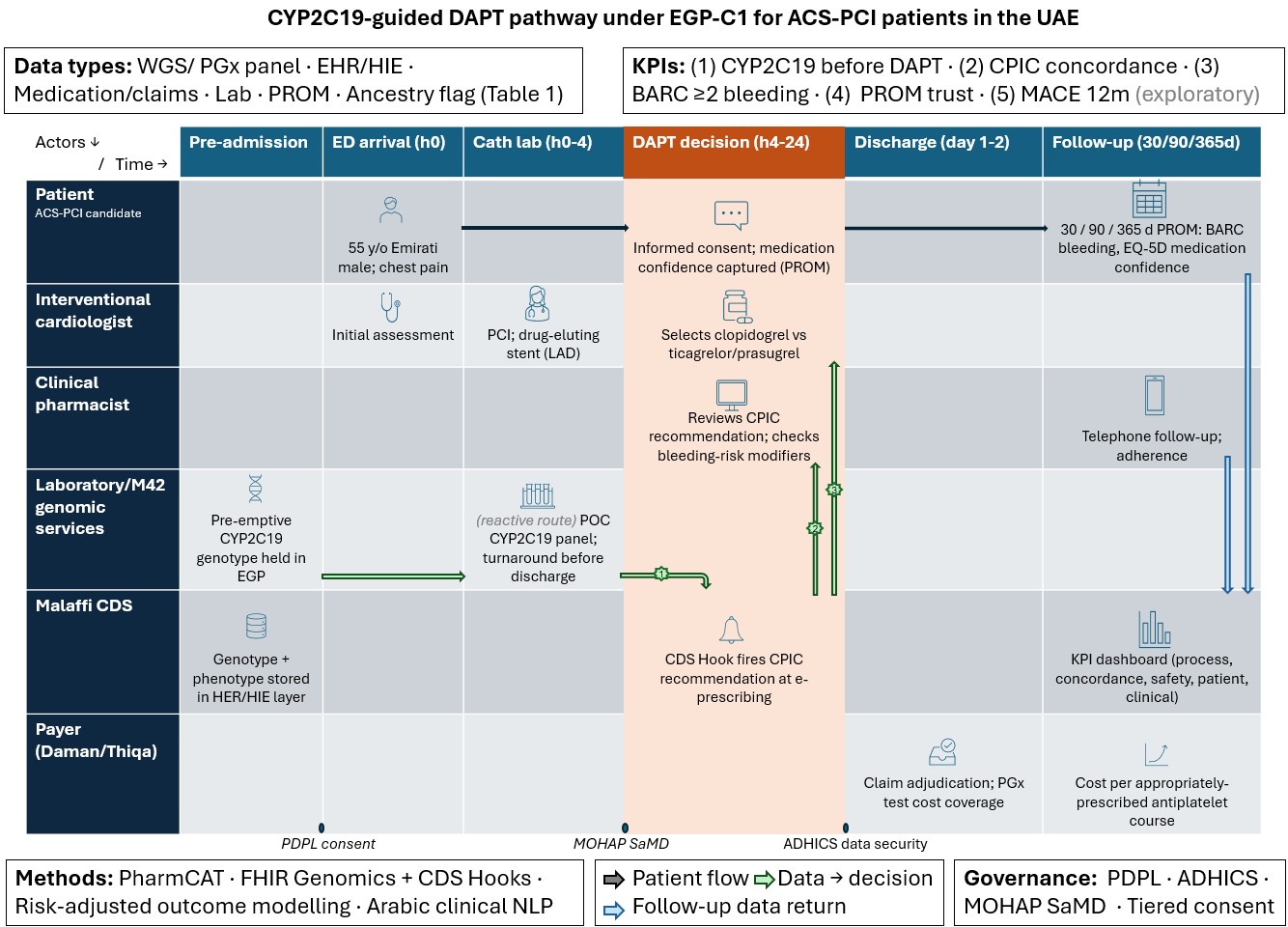
Figure 1. The CYP2C19-guided dual antiplatelet pathway under the proposed EGP-C1 pilot.
Rows are actors, columns are time, data converges at the prescribing decision, and the governance
gates (data protection, security, medical-device approval) sit between stages.
A six-row data fabric
Sound decision support needs more than a genotype. Six data types converge into one
decision-grade record:
- Genomic. The CYP2C19 genotype, translated to a metaboliser phenotype.
- EHR and health-information-exchange. The channel that carries the recommendation to the prescriber at the point of care.
- Medication and claims. What was actually prescribed and taken, and adherence over the year.
- Laboratory. Renal and bleeding-risk modifiers that refine the drug choice beyond the gene.
- Patient-reported outcomes. Bleeding events, quality of life, and confidence in the medication.
- Demographic and ancestry. Context for fair phenotype interpretation in an under-represented population.
Methods
Four health data science methods turn the fabric into a working tool. CPIC star-allele
translation with PharmCAT calls the phenotype. Rules-based decision support delivers the
recommendation at e-prescribing through HL7 FHIR Genomics and CDS Hooks. Risk-adjusted outcome
modelling checks whether the pathway actually changes outcomes. Arabic clinical natural language
processing reads bleeding and adherence signals out of free-text notes.
Governance
None of this runs without governance, which is often where clinical-AI plans quietly fail. The
plan maps the UAE data-protection law, the ADHICS security standard, and the
Software-as-a-Medical-Device pathway that a prescribing tool would have to clear before it could
touch a patient.
The recommendation
The recommended next step is EGP-C1, a twelve-month feasibility pilot rather than an outcomes
trial. It would run in two Abu Dhabi centres with 500 to 1,000 patients, measured against five
KPIs covering process, prescribing concordance, safety, patient experience, and an exploratory
clinical outcome. The full plan, the data-fabric table, and the references are in the
repository.